

What is being tested?
Escherichia coli (E. coli) bacteria commonly occur in nature and are a necessary component of the digestive process. Most strains of E. coli are harmless, but disease-causing (pathogenic) E. coli can cause inflammation of the stomach and intestines (gastroenteritis). Laboratory tests can detect the presence of pathogenic E. coli that produce Shiga toxins.
Multiple subtypes of E. coli cause diarrheal illness, and they are classified by how they cause the disease. For example, some invade the lining of the intestines, causing inflammation, while others produce toxins.
E. coli that produce poisons called Shiga toxins are generally the only type of E. coli that are tested for in clinical settings from stool specimens. The Shiga toxins associated with these infections are so called because they are related to the toxins produced by another type of disease-causing bacteria, Shigella. Shiga toxin-producing E. coli (STEC) may also be called verocytotoxic E. coli (VTEC) or enterohemorrhagic E. coli (EHEC).
A strain of STEC called O157:H7 is the STEC strain responsible for most gastrointestinal illness outbreaks in the U.S. However, non-O157 strains of STEC are gaining recognition, in part due to increased testing for them by clinical laboratories. For example, a 2011 outbreak of E. coli O104:H4, a non-O157 STEC, was associated with travel to Germany and resulted in 32 deaths related to contaminated sprouts. According to the Centers for Disease Control and Prevention, STEC O157 causes about 36% of STEC infections in the U.S., while non-O157 STEC cause the rest.
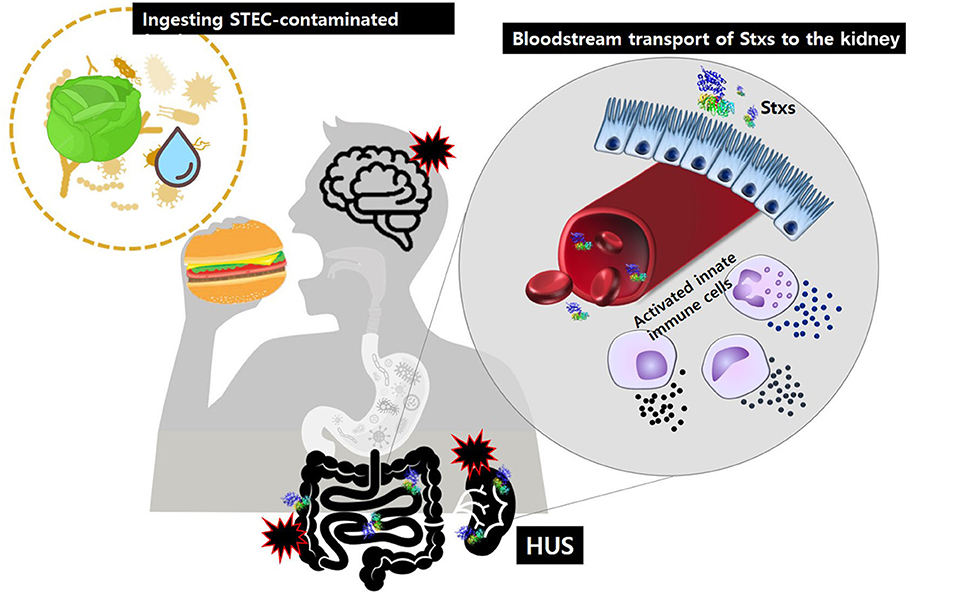
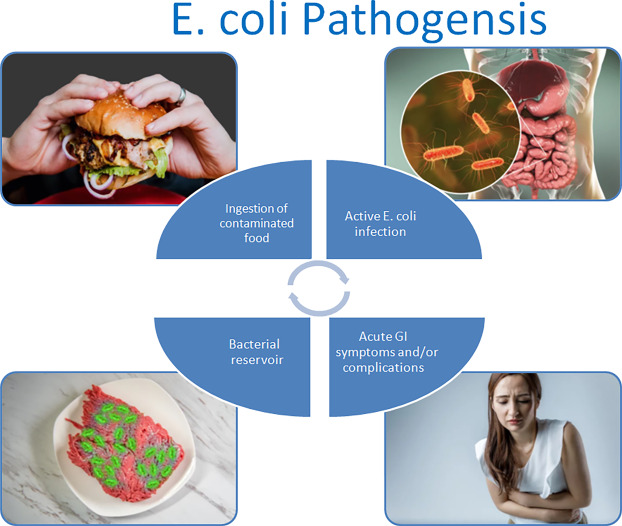
Outbreaks have been linked to the consumption of contaminated food, including undercooked ground beef, unpasteurized juice, unpasteurized milk, and raw produce such as leafy greens and alfalfa sprouts. STEC may also be transmitted through contaminated water, contact with farm animals or their environment, and from person to person. Even ingesting small numbers of E. coli can cause an infection.
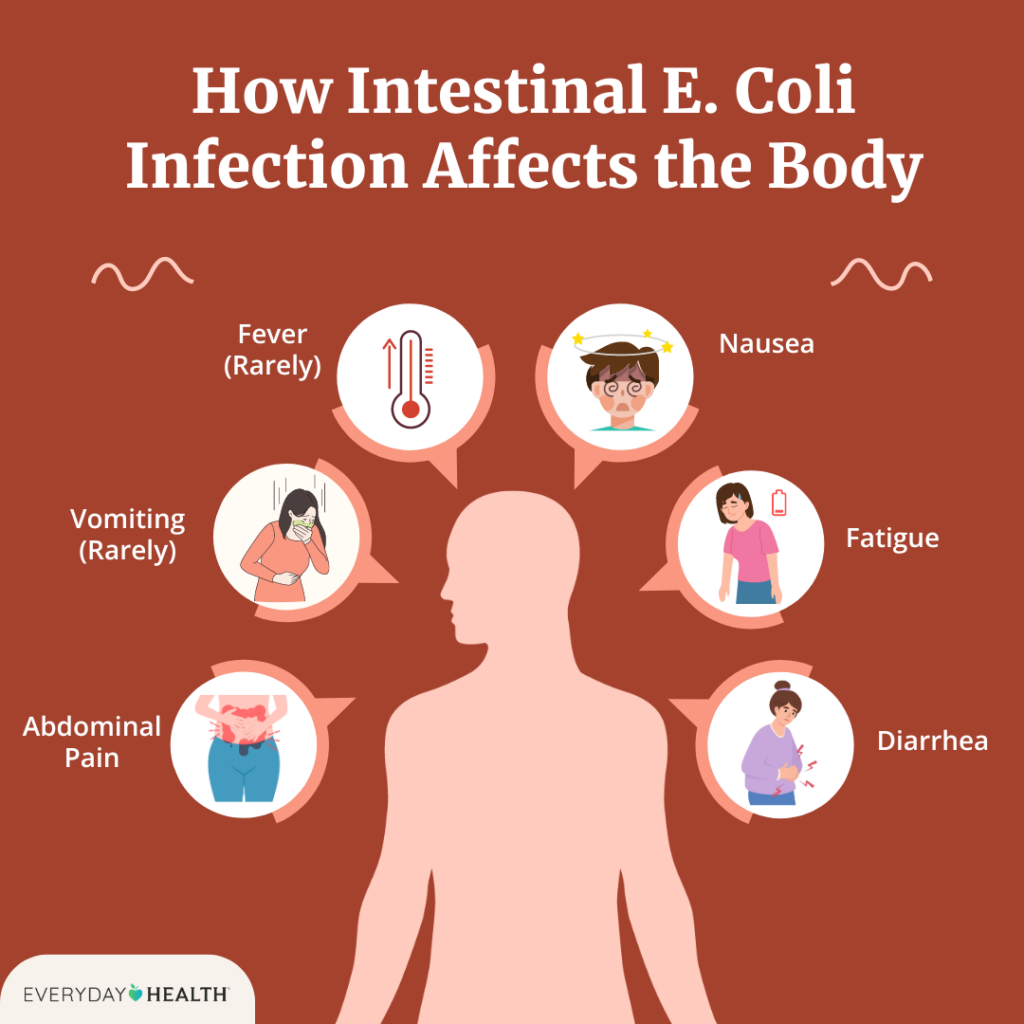
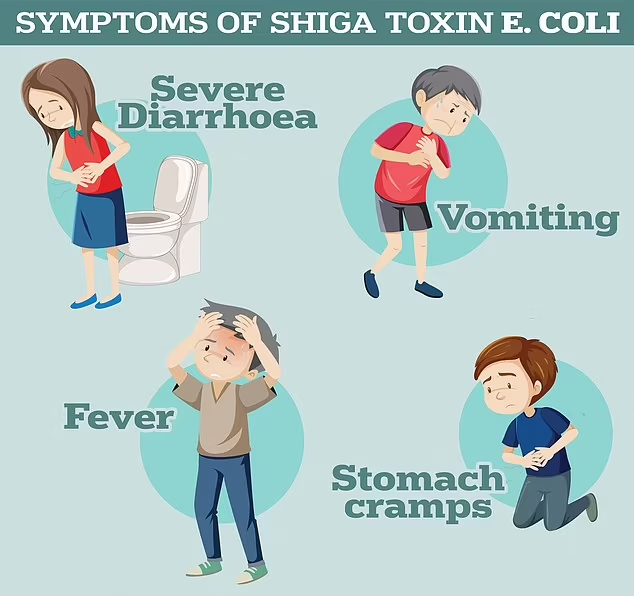
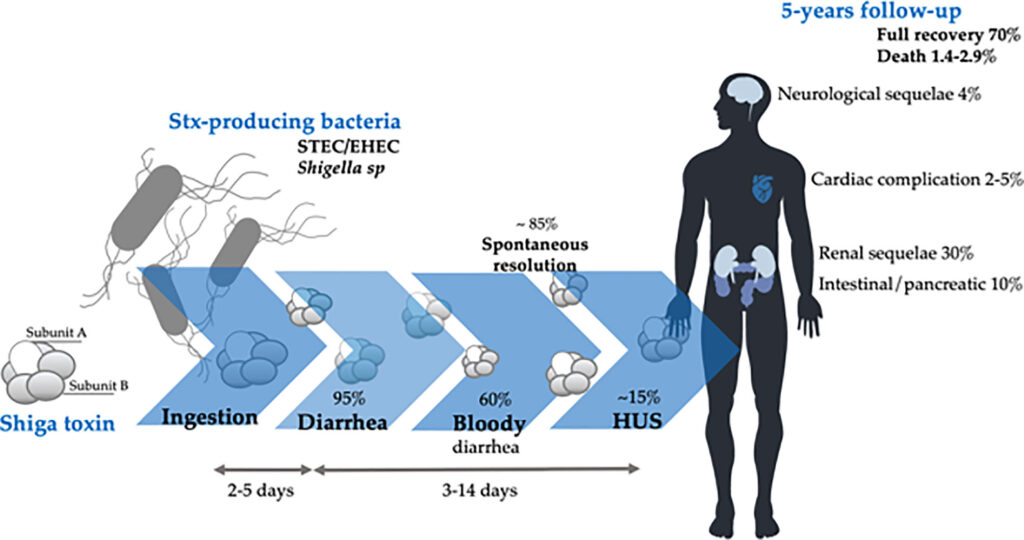
In addition to symptoms of nausea, severe abdominal cramps, watery diarrhea, fatigue, or possible vomiting and low-grade fever, STEC infections are often associated with bloody stools and, less commonly, can lead to serious complications, specifically hemolytic uremic syndrome (HUS). HUS is a result of the toxin entering the blood and destroying red blood cells (hemolysis). It can lead to kidney failure (uremia or the build up of nitrogen wastes in the blood) and can be life-threatening. Signs and symptoms include decreased frequency of urination (evidence of uremia), fatigue, and pale skin due to hemolytic anemia. HUS usually develops about a week after the onset of diarrhea.
About 5-10% of people who are diagnosed with an O157 STEC infection develop HUS. Children, the elderly, and persons with weakened immune systems are at greatest risk. However, most healthy persons recover from a STEC infection within a week and do not develop HUS. Non-O157 Shiga toxin-producing E. coli can cause the same symptoms and complications and likely account for 20-50% of STEC infections in the U.S. annually. Different testing techniques are required to identify O157 and non-O157 Shiga toxin-producing E. coli.

How is the sample collected for testing?
A fresh liquid or unformed stool sample is collected in a clean, dry container. The stool sample should not be contaminated with urine or water. Once it has been collected, the stool should be taken to the laboratory immediately or refrigerated and taken to the lab as soon as possible. Some laboratories provide transport media to support the survival of the organism from the time of collection until delivery to the laboratory. STEC becomes difficult to detect in the stool after one week of illness, so the timing of sample collection relative to the onset of illness is important.
Shiga toxin, secreted by Shigella dysenteria, and Shiga-like toxins (Stx1 and Stx2) secreted by E. coli and other bacteria, are still a problem in infectious diseases (Karmali, 2004; Palermo et al., 2009; Sandvig, 2006). During recent years there seems to be an increasing problem with food contaminated with E.
STEC infection is an infection caused by certain Escherichia coli (E. coli) bacteria. These bacteria are germs that naturally live in the intestines and feces (poop) of many animals, especially farm animals (such as cows, goats, and sheep) and deer
PCR TEST

PCR assays to detect the stx1 and stx2 genes are used by many public health laboratories for diagnosis and confirmation of STEC infection. Depending on the primers used, these assays can distinguish between stx1 and stx2 (76–78). Assays also have been developed that determine the specific O group of an organism, detect virulence factors such as intimin and enterohemolysin, and can differentiate among the subtypes of Shiga toxins (79–81). Because these tests are not commercially available, they are rarely used for human disease diagnosis in the United States.
Most PCR assays are designed and validated for testing isolated colonies taken from plated media; some assays have been validated for testing on stool specimens subcultured to an enrichment broth and incubated for 18–24 hours. Shiga toxin PCR assays on DNA extracted from whole stool specimens are not recommended because the sensitivity is low (82). The time required to obtain PCR assay results ranges from 3 hours (if an isolate is tested) to 24–36 hours (if the specimen is first subcultured to an enrichment broth or plate).
DNA-based Shiga toxin gene detection is not approved by FDA for diagnosis of human STEC infections by clinical laboratories; however, public health laboratories might use this technique for confirmatory testing after internal validation. One commercial PCR kit is available to test for STEC virulence genes (DEC Primer Mix, Mira Vista Diagnostics, Indianapolis, Indiana); however, this test is labeled for research use only, can only be used on isolates, and is not approved by FDA for diagnosis of human STEC infections. Clinical laboratories that are considering adding a DNA-based assay to their testing options need to establish performance specifications for the assay as required by CLIA (59), and reports from such testing should include a disclaimer to inform clinicians that the test is not approved by FDA (83). No commercially available proficiency testing programs are available in the United States for PCR assays that target the Shiga toxin genes; however, internal proficiency testing events and exchanges with other laboratories may be used to fulfill CLIA requirements
Shiga toxin–producing E. coli (STEC) cause approximately 100,000 illnesses, 3,000 hospitalizations, and 90 deaths annually in the United States, according to the last estimate in 1999 (2). Most reported STEC infections in the United States are caused by E. coli O157:H7, with an estimated 73,000 cases occurring each year (2). Non-O157 STEC bacteria also are important causes of diarrheal illness in the United States; at least 150 STEC serotypes have been associated with outbreaks and sporadic illness (2–4). In the United States, six non-O157 serogroups (O26, O45, O103, O111, O121, and O145) account for the majority of reported non-O157 STEC infections (5).

The toxins produced by STEC were named based on their similarity in structure and function to Shiga toxins produced by Shigella dystenteriae type 1 (6). Shiga toxin 1 (Stx1) is neutralized by antibodies against Shiga toxin, whereas Shiga toxin 2 (Stx2) is not neutralized by antibodies against Shiga toxin but is neutralized by homologous antibodies. STEC are also referred to as verocytotoxigenic E. coli; STEC that cause human illness are also referred to as enterohemorrhagic E. coli. In this report, all E. coli that produce a Shiga toxin are referred to as STEC. STEC serotypes are named according to their somatic (O) and flagellar (H) antigens. In this report, all STEC with the O antigen 157 are referred to as O157 STEC, regardless of whether the H7 antigen has been identified or Shiga toxin production has been confirmed. STEC with other O antigens are referred to as non-O157 STEC or by their specific O antigen.
STEC infection causes acute, often bloody, diarrhea. Approximately 8% of persons who receive a diagnosis of O157 STEC infection develop hemolytic uremic syndrome (HUS), a life-threatening condition characterized by thrombocytopenia, hemolytic anemia, and renal failure (7–9). Thrombotic thrombocytopenic purpura (TTP), a syndrome with signs and symptoms that are similar to those of HUS, is typically diagnosed in adults. When TTP is diagnosed after a diarrheal illness, the condition is usually caused by infection with O157 STEC or another STEC. In this report, regardless of the age of the patient, TTP diagnosed after a diarrheal illness is referred to as HUS (10).
Whether an illness progresses to HUS depends on strain virulence and host factors (11). Although most persons with diarrhea-associated HUS have an O157 STEC infection, certain non-O157 STEC strains also can lead to HUS (3). The virulence of non-O157 STEC is partly determined by the toxins they produce; non-O157 STEC strains that produce only Stx2 are more often associated with HUS than strains that produce only Stx1 or that produce both Stx1 and Stx2 (12). STEC infections and HUS occur in persons of all ages, but the incidence of STEC infection is highest in children aged <5 years, as is the risk for HUS (9). Although STEC infections are more common during summer months, they can occur throughout the year.
STEC transmission occurs through consumption of a wide variety of contaminated foods, including undercooked ground beef, unpasteurized juice, raw milk, and raw produce (e.g., lettuce, spinach, and alfalfa sprouts); through ingestion of contaminated water; through contact with animals or their environment; and directly from person to person (e.g., in child-care settings). Both O157 STEC and O111 STEC have a low infectious dose (<100 organisms) (13); the infectious dose of other serogroups is not known.
Prompt and accurate diagnosis of STEC infection is important because appropriate treatment with parenteral volume expansion early in the course of infection might decrease renal damage and improve patient outcome (14). In addition, because antibiotic therapy in patients with STEC infections might be associated with more severe disease, prompt diagnosis is needed to ensure proper treatment. Furthermore, prompt laboratory identification of STEC strains is essential for implementation of control measures, for effective and timely outbreak responses, to detect new and emerging serotypes, and to monitor trends in disease epidemiology (1,15,16).
Most O157 STEC isolates can be readily identified in the laboratory when grown on sorbitol-containing selective media because O157 STEC cannot ferment sorbitol within 24 hours. However, many clinical laboratories do not routinely culture stool specimens for O157 STEC. In addition, selective and differential media are not available for the culture of non-O157 STEC, and even fewer laboratories culture stool specimens for these bacteria than for O157 STEC.

Recently, the increased use of enzyme immunoassay (EIA) or polymerase chain reaction (PCR) to detect Shiga toxin or the genes that encode the toxins (stx1 and stx2) has facilitated the diagnosis of both O157 and non-O157 STEC infections. Although EIA and other nonculture tests are useful tools for diagnosing STEC infection, they should not replace culture; a pure culture of the pathogen obtained by the clinical laboratory (O157 STEC) or the public health laboratory (non-O157 STEC) is needed for serotyping and molecular characterization (e.g., pulsed-field gel electrophoresis [PFGE] patterns), which are essential for detecting, investigating, and controlling STEC outbreaks.
Simultaneous culture of stool for O157 STEC and EIA testing for Shiga toxin is more effective for identifying STEC infections than the use of either technique alone (17,18). Because virtually all O157 STEC have the genes for Stx2 (stx2) and intimin (eae), which are found in strains that are associated with severe disease (5,12,19–22), detection of O157 STEC should prompt immediate initiation of steps such as parenteral volume expansion to reduce the risk for renal damage in the patient and the spread of infection to others.
Guidelines for clinical and laboratory identification of STEC infections have been previously published (1); this report provides the first comprehensive and detailed recommendations for isolation and identification of STEC by clinical laboratories. The recommendations are intended primarily for clinical laboratories but also are an important reference for health-care providers, public health laboratories, public health authorities, and patients and their advocates.
What does Shiga toxin do to the body?
How long does Shiga toxin E. coli last?
What food is commonly linked to Shiga toxins?
Infection most typically occurs by eating contaminated food, particularly raw or undercooked meat. Infection can also occur after eating any product contaminated with STEC, including lettuce, alfalfa sprouts, salami, and raw (unpasteurized) milk, juice, or cider.
What are the symptoms of a STEC infection?
How does E. coli spread from person to person?




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}